When it comes to answering “Should you vaccinate your child for COVID?”, there are 3 major errors in the messaging.
I’m not here to convince you to (or to not) vaccinate your child under 5 for COVID.
I AM here to clear up these misconceptions.
So you have transparent information without fear or emotion. So you can be comfortable making an informed decision for YOUR child.
Because – healthy kiddos + peace of mind – isn’t that parental bliss?
***I dug into both FDA Reports – so you wouldn’t have to. Let me know your Qs***
TL;DR – 3 Biggest Myths about COVID Vaccines in Kids
**based on truly digging into the data** (see below TL;DR for details)
Myth #1: COVID doesn’t make healthy kids sick / flip-side: COVID is the #4 leading cause of death for kids
TRUTH: The news (and even the CDC has mis-stated this one badly) – but myths come from both sides of the aisle. The actual cumulative # of deaths in children under 5 attributed to COVID is 273, from 2020 – present. BUT – 50% of those had no prior medical conditions.
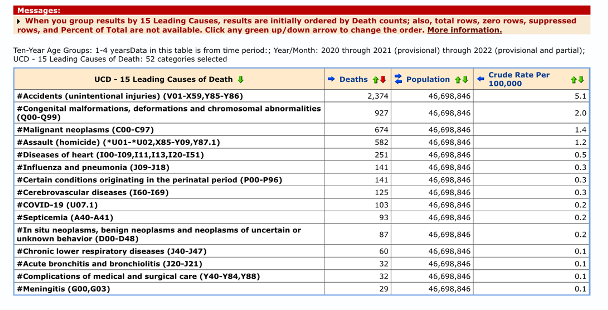
In terms of cause of death for ages 1-4, it ranks at #9, behind accidents, birth-related conditions, assault, and others.
That doesn’t mean COVID is harmless – in fact as an ER doctor, I can attest to the fully uncontrolled and unpredictable way COVID can ravage the body. It just means that the truth is in the middle.
Myth #2: (efficacy myths): “Moderna is less effective”… or an alternate headline.. “Pfizer was only done in 10 kids”
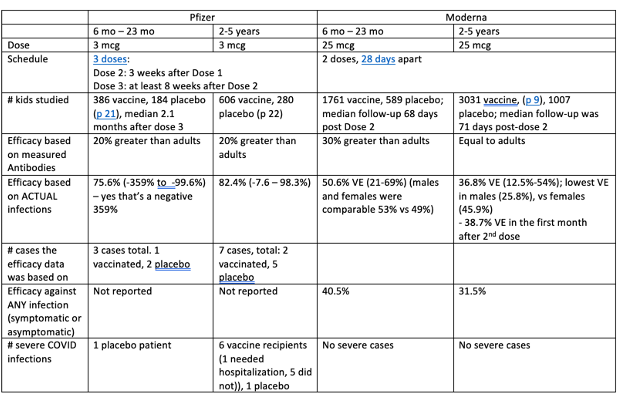
TRUTH: The headlines make it sound like Pfizer was far more effective than Moderna – “Pfizer is 80% effective, while Moderna is 37-50%!”. BUUUT – (1) In this data of real cases, Pfizer only had 10 positive cases to base these numbers (Moderna had 170 cases). That gives me more faith in the Moderna data in terms of efficacy. In fact, the FDA even said that the Pfizer analysis was not reliable, since it was based on so few cases.
Myth 2b: “Pfizer is 3 doses” – TRUTH: Actually, both of these will likely have a booster. Moderna is working on an omicron-specific booster, and Pfizer in their FDA filing noted they’d be applying for a 4th shot.
Myth 2c: The vaccines aren’t effective – everyone I know who was vaccinated got COVID!
TRUTH: Think of this like a seatbelt: it doesn’t guarantee you won’t be in an accident – they significantly cut your risk that if you are, you’ll be seriously injured. Vaccines are similar – as the data has shown. While vaccines have been shown to reduce non-serious infection by only about 20-30%, but reduce hospitalization in kids by 68%, and critical illness by 79%.
Myth #3: COVID Vaccine causes myocarditis.
TRUTH: While there is a risk of myocarditis from COVID vaccine, studies consistently show that your risk of myocarditis is significantly (think between 6-16x and sometimes even more) higher risk of myocarditis after a COVID infection, than after a vaccine. Plus, myocarditis after a COVID vaccine is typically milder than myocarditis from COVID.
**Moderna does have approximately 2x the risk of myocarditis than Pfizer, which is why I do recommend Pfizer for young males (see below).
Overall: Based on the data above, some parents may choose to vaccinate, some to wait to match the vaccine timing to back-to-school / peak cold and flu and covid season, and some may choose to not vaccinate at this moment. I think that all – as long as they are made from an informed standpoint – can be valid, and that when we understand the actual data, we can better trust the science, and our own decisions.
For males ages 12-30: I DO recommend (1) giving Pfizer due to lower incidence of myocarditis, and (2) spacing doses 8 weeks apart, since risk of myocarditis was most common in doses 21 days apart.
PLUS, some GOOD NEWS. We can ALL be elated that vaccines are finally available in this age group. It means we can get back to normalcy. Read the ending for why this is SUCH good news for us as a country – whatever you decide as an individual family.
In which case, COVID goes from being a world disruptor, to a bug that we learn to live with; less quarantines, less masking, less fear.
And that’s a new normal that I’m happy to accept.
FULL REPORT: The 3 worst headline errors on if you should vaccinate your child for covid
MYTH #1: MEDICAL NEED: “KIDS DON’T GET SICK” (OR ON THE FLIP-SIDE), “COVID19 IS THE #1-4 CAUSE OF DEATH IN LITTLES”.
Anyone have whiplash?
First, you need to know – “What is the ACTUAL risk of COVID-19 to my child?”
It’s impossible to make the decision when you’re not getting straight answers here – and generalization and sound-bytes just don’t help. In addition, a recent publication that was cited by the FDA VRBPAC and CDC ACIP even was incorrect.
Risks of COVID include death rates of course, but also hospitalizations, myocarditis, and MIS-C.
How many children have died from COVID from 2020 – 2022 (TOTAL)
- Total Deaths WITH COVID (unclear if it was the cause): 449
- children < 5 months: 227
- Children 5 months – under 5 years: 222
- Deaths Directly Attributed to COVID: 278
- Children < 1 year: 175
- Children 1-4 years: 103
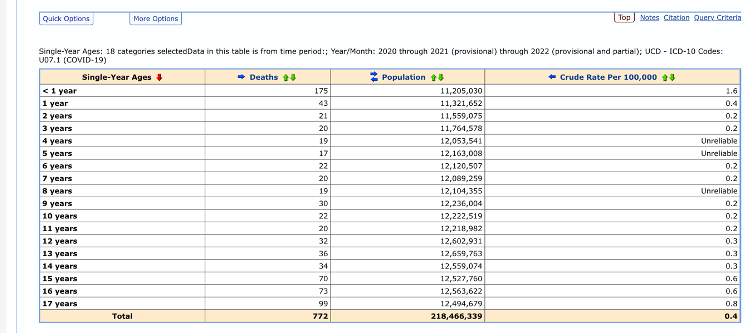
Another way to look at it – where does COVID rank in terms of causes of death? Many headlines have recently noted it as #4- it’s actually #9. And, as you can see, the 103 deaths from COVID are still starkly lower than other causes of death, such as accidents (drownings, fires, car accidents) that come in at #1.
Of course, we also look at other outcomes besides death:
- MIS-C – a total of 8,525 children have developed MIS-C, accounting for 69 deaths. The median age was 9 years, with half of them 5-13.
- Hospitalizations – around 210 / 100,000 children under 5 have been hospitalized for COVID. While about half of those being children without any chronic medical condition. When you factor in that children with chronic medical conditions represent about 12-18% of the total pediatric population, it’s clear that they carry a disproportionate risk, but that healthy children are not at all immune.
- Myocarditis – (I’ll go in DEPTH about the risk of myocarditis from infection, below. Just know that COVID does increase the risk of myocarditis, simply after infection (which is often included as part of the MIS-C condition).
- Long-COVID – While we still don’t fully understand long COVID, nor how a frequent it is, a number of cases have written about long-COVID in children.
Overall, speaking here as an ER doctor, the challenge immunologically is the scale and unpredictability with which COVID hits the body. It both suppresses the immune system while also triggering it into overdrive. It causes blood clots, triggers fatigue, and other long-term symptoms. All of that makes the idea of a more controlled, small “dose” of COVID (ie a vaccine) a much more desirable option.
MYTHS #2: EFFICACY – EFFICACY: “MODERNA IS LESS EFFECTIVE THAN PFIZER.” “PFIZER’S STUDY WAS ONLY IN 10 KIDS”, “PFIZER IS 3 DOSES”
Oh – SO much here. And with good reason – 500 pages of FDA reports that most people have not read is a primed environment for soundbites!
Efficacy background: When we think about the vaccine, there is the percent reduction to (1) death, (2) hospitalization, and (3) symptomatic illness.
Now, call me callous, but as an ER doctor, I don’t really care if your child gets COVID – at least from their physical health standpoint (yes their missing school and your sanity for staying home count). I don’t care, IF – IF they’re home, if they’re well, and not hospitalized and not giving COVID to someone who is medically vulnerable. If they’re sitting home and sucking on a lollipop and watching Bluey, and not in the ICU or hospital, that’s a win.
How much do the vaccines do that?
VACCINE EFFICACY:
Reduce symptomatic (non-severe) infection: This is where they’re weakest – but if I had to choose, this is where I least mind that. As low as a 30% reduction in symptomatic cases by 2 months after vaccination (in omicron), some places reporting a 20% reduction in non-critical cases.
Reduce hospitalizations, severe cases, and death: THIS is what matters, and the vaccines show a 79% reduction against critical illness, and a 68% reduction in hospitalizations in kids 5-11.
Think of COVID vaccines like your car seatbelt – it doesn’t guarantee that you won’t die / be injured in a car accident, but that seat belt cuts your risk by 50%. (And a COVID vaccine does even more).
EFFICACY BY VACCINE:
- Moderna has faster time to immunity
- Pfizer efficacy doesn’t seem to truly kick in until after the 3rd Even in the 2 cases of COVID (out of 7) in the 2-5 year old’s, the 2 were after their 2nd dose, but before their 3rd.
- On the flip-side, kids who get Moderna get some immunity after even the 1st Then, kids reach peak efficacy after the 2nd dose (4-8 weeks after the first).
- Moderna was based on real COVID diagnoses, but Pfizers number of cases were much smaller.
- While Pfizer’s numbers sound great (82.4% efficacy!!) they were based on 7 positive cases of COVID, and I don’t think we can legitimately know their full efficacy yet. Even the FDA said that this analysis “was determined not to be reliable due to the low number of COVID-19 cases that occurred in study participants”
- Pfizer doesn’t reach its peak efficacy until after the 3rd dose – meaning after 3 months.
- Moderna does have more side effects.
- Just like we see in older children, Moderna has a higher incidence of side effects. This is at least partly because their dose is so much higher.
- What about prior COVID infection?
- Hybrid immunity, or what happens if you’ve had a COVID infection AND at least one dose of a vaccine, appears to be more protective than either infection or vaccine alone. Think of a vaccine after infection as a “booster”. I typically, however, suggest waiting 8 weeks after infection before the vaccine, since a child already has some immunity on board, and to minimize side effects.
- Unfortunately, neither Pfizer nor Moderna had enough cases among participants with prior COVID infection to estimate hybrid infection / vaccine efficacy (p 11) – so the above comments on hybrid immunity are speculation, but based on effects in older children and adults.
Oh and about the doses? Moderna will likely add a booster (which is aiming to be Omicron specific), and parents need to also know that Pfizer will likely also become a FOUR-SHOT series. In their report, Pfizer wrote that “it is likely that a booster dose will be needed in addition to the three-dose primary series.” Four shots in littles is a lot – and something of which parents should be made aware.
MYTH #3: COVID VACCINES IN KIDS CAUSE MYOCARDITIS (AND IN GENERAL ARE NOT SAFE)
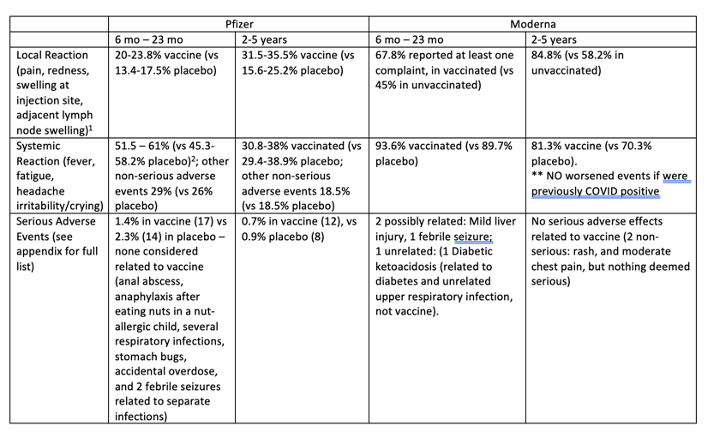
What were the side effects? The most common side effects were mild (pain at injection site, crying, fever that resolved) – see the below table I created for specifics.
MYOCARDITIS
The Pfizer study had no incidence of cardiomyopathy (ie dysfunctional heart condition, including myocarditis and pericarditis). Moderna had one child with shortness of breath and one with chest pain – both were checked and had no cardiomyopathy. That’s reassuring, but still the numbers of children getting the vaccine would need to be in the hundreds of thousands for us to see if any cases. So, for more insights, I’m showing data from the HIGHEST risk group for myocarditis, males 18-29. This allows you to compare, and to also know that all other ages will have even lower risks across the board.
For one, when we talk about myocarditis, males 18-29 just seem to get it more often in general (even before COVID). We don’t exactly understand the pathology – but it’s important for understanding why they also get myocarditis from COVID more than other groups.
| Risk of Myocarditis |
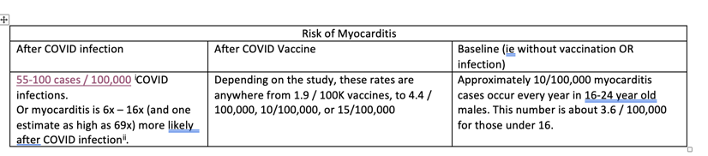
SOO – whichever numbers you look at, from various studies, you see that:
- COVID infection causes the biggest amount of myocarditis.
- The rates of myocarditis from the vaccine (even if you look at MANY studies, as I have done), is far less than the myocarditis from COVID. Myocarditis due to COVID tends to be relatively mild.
- Myocarditis is greatest in males 18 and up (as low as 12 years), particularly after the 2nd dose of COVID vaccine, and particularly when the doses are given 21 – 28 days apart. This is why many (myself included) recommend waiting 8 weeks between doses 1 and 2 of your COVID vaccine for this age group. It’s also why I tend to recommend waiting 8 weeks after infection, before vaccinating.
- Of note, Moderna does tend to be about 2x higher risk of myocarditis than Pfizer – which is why – especially in boys 11 and up, Pfizer is likely a better choice.
This isn’t surprising, when you think of myocarditis as an inflammatory phenomenon. So, anything that causes total body inflammation (ie, COVID), can lead to myocarditis. Why there is also myocarditis from the COVID vaccine isn’t entirely clear – likely due to the inflammation that exists; but the bottom line is that it is less than the inflammation from COVID.
FERTILITY
The COVID vaccine and fertility was an early fear – but this is one that we can entirely put to rest. It was largely based on a concept that was just not biomedically sound – and now we have evidence to confirm that.
In one study looking at couples trying to get pregnant, they found that COVID vaccination status had no impact on conception. However, while COVID infection did not significantly impact conception, male COVID infection was possibly associated with a reduction in ability to conceive for 60 days. In another, the miscarriage rate among pregnant women receiving the COVID vaccine was consistent with typical miscarriage rates, with the same finding in this study from Switzerland.
PULLING IT TOGETHER – SHOULD YOU VACCINATE YOUR CHILD FOR COVID?
You know that I usually like to be able to really give you a single, distinct answer, as much as I can. However, that’s really harder in this age group.
Here’s how you can make this decision.
Safety: From a safety standpoint, I have very little concern about this vaccine. The only caveat to that is that in boys 12 and up, I’d recommend giving the 2nd dose 8 weeks after the first, to minimize any risk of myocarditis.
MEDICAL NEED: ASK YOURSELF THESE 3 QUESTIONS FOR YOUR CHILD
- What is the risk to them (looking at the child illness rates above, hospitalizations, etc., and keeping in mind that half of children hospitalized had no medical problems)
- What is the risk to someone in the home? I feel confident saying that if a vaccine reduces symptomatic infection by 30-40%, plus, also reduces severe infection, and reduces length of time of being infected, that child will spread the virus less. And I would argue that the risk to a child of gravely sickening an already fragile loved one, would be greater than any risk of vaccination to the child.
- How much does vaccination allow your child to go back to *life*? To go back to no vaccines, not quarantining, and less school missed because they’re sick? How you view these things, will also affect your decision.
If your answer to any of those 3 questions is “a lot”, or “more risk than I’m willing to tolerate”, then given the reassuring safety profile of the vaccine, it makes absolute sense to go ahead and vaccinate them – but now you can do so from an informed stance.
I also think many parents will choose not to vaccinate their littles. I don’t think this is an entirely unreasonable decision, if their answers to the 3 questions above are “not much at all”.
WHICH VACCINE WOULD I CHOOSE?
If you’re choosing to vaccinate your child, then I’d likely suggest Moderna. We know they get efficacy early on – and that we have real-world data. The only exception here would be if a child is on the young side (less than 2), then I’d talk with your pediatrician to see if they think a smaller dose (ie Pfizer) would be sufficiently protective. The two different doses allows parents to make a judgment call based on their child’s size (even if that’s not really the way they were intended).
The one situation in which I’d opt for Pfizer is in the kiddos older than 11, especially in boys – in that case, I’d suggest Pfizer over Moderna (due to the lower risk of myocarditis) and still space them 8 weeks apart.
In terms of timing, I also think it’s ok if parents want to time the vaccines to peak just in time for school starting, or for the typical cold/flu/covid peak in late fall.
AND some Good News:
WHAT DOES THE FUTURE LOOK LIKE FOR COVID AND KIDS?
I’ll end with a positive note, in part brought up by my conversation with Dr. Paul Offit, Director of the Vaccine Education Center at Children’s Hospital of Philadelphia and member of the FDA Vaccines and Related Biological Products Advisory Committee, now that vaccinations are available for almost all our population (all but the under 6 months), the higher natural + vaccinated community immunity we are reaching, and the expansion of effective therapies, that COVID will become circulating and, endemic, but not disruptive. Dr. Offit suggested that going forward, if a child were symptomatic, they could be tested, and kept at home if positive, then able to return to school 24 hours after symptoms end – much like we do for other respiratory viruses.
In which case, COVID goes from being a world disruptor, to a bug that we learn to live with; less quarantines, less masking, less fear.
And that’s a new normal that I’m happy to accept.
All my best,
Dr. Darria
Thank you to Dr. Paul Offit for his time and graciousness in answering questions, and for Kelley of COVID-Georgia for your help digging through the mortality data.